See pulmonary embolism in pregnancy for pregnancy specific information.
Background
Pulmonary embolism is an obstruction of one of the branches of the pulmonary arteries by material; typically a thrombus
- Fat, Air, and tumor embolisms can similarly and obstruct a branch of the pulmonary artery, but are not covered in this section
- A pulmonary embolism is on the spectrum of Venous thromboembolism (VTE)
- Most emboli are thought to arise from lower extremity proximal veins (iliac, femoral, and popliteal), whereas a thrombus of the distal veins (calf) resolves spontaneously ⅔ of the time [1] [2] [3]
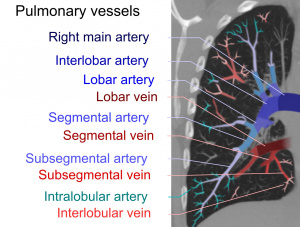
Pulmonary emboli can be classified according to the level along the pulmonary arterial tree.
Epidemiology
- In the US, approximately 370,000-390,000 PE’s are diagnosed annually [4] [5]
- Mortality
- Hemodynamically stable (AHA/ACC Class A & B or ESC Low Risk) patients with a PE have a direct mortality of about 1%, however hemodynamically unstable patients mortality ranges from 25-50% [6]
- For almost one quarter of PE patients, the initial clinical presentation is sudden death [7]
Clinical Features
- Diagnosis of PE is challenging, with less than 10% of patients evaluated for a PE ultimately diagnosed with a PE [8]
Symptoms
Signs
- Tachycardia (HR>100), Tachypnea (RR>20), Hypoxemia (SpO2<95%) are seen ~50% of the time
- Hypotension (SBP<90) only seen 10% of the time, but largest predictor of mortality
- Unilateral calf tenderness or edema, suggestive of a DVT
- Other signs may include accentuated pulmonic component of second heart sound, JVD, or decreased breath sounds
Differential Diagnosis
Critical
Emergent
Nonemergent
Emergent
- Pulmonary
- Cardiac
- Other Associated with Normal/↑ Respiratory Effort
- Other Associated with ↓ Respiratory Effort
Non-Emergent
Workup
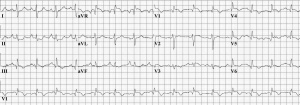
ECG of a person with pulmonary embolism, showing sinus tachycardia of approximately 100 beats per minute, large S wave in Lead I, moderate Q wave in Lead III, inverted T wave in Lead III, and inverted T waves in leads V1 and V3.
Assessing Pretest Probability
- A thorough H&P is paramount to assess probability of PE
- Objective scoring systems (Wells, revised Geneva) performs similarly to experienced clinician gestalt in assessing pretest probability[9] [10]
If pretest probability of PE is low (<15%)
- Assess PERC Rule criteria,
- If all criteria are "No", very low probability of PE, and no further testing is required
- However, if even 1 criteria is met, proceed as if patient is of intermediate risk
If pretest probability of PE is intermediate (15-50%), or unable to rule out with PERC:
- Perform d-dimer testing and assess YEARS criteria
- 0 YEARS criteria and d-dimer <1000ng/mL
- ≥1 YEARS criteria and d-dimer <500ng/mL, or age adjusted threshold
- 0 YEARS criteria and d-dimer >1000ng/mL
- PE not excluded, perform diagnostic imaging
- ≥1 YEARS criteria and d-dimer ≥500ng/mL, or age adjusted threshold
- PE not excluded, perform diagnostic imaging
If pretest probability of PE is high (>50%)
- Perform diagnostic imaging
Diagnosis
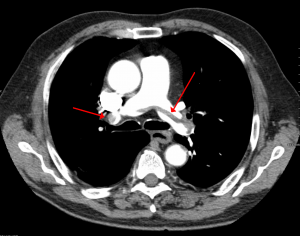
A large pulmonary embolism at the bifurcation of the pulmonary artery (saddle embolism).
Diagnostic Imaging
- Computed Tomography Pulmonary Artery (CTPA) is the standard and preferred imaging modality
- If a CTPA is unable to be obtained, a high probability ventilation/perfusion (V/Q) scan is sufficient
- V/Q Single-photon emission computed tomography (SPECT) is preferred over a planar V/Q scan
- SPECT combines a non-contrast CT with a planar V/Q and has equivalent sensitivity to CTPA [11]
Additional diagnostic tools
Labs
- Typically obtained to rule out other conditions and to help with risk stratification
- Important to include troponin, BNP, lactate
- Elevated troponin has a pooled OR of 4.33 for mortality [12]
- Elevated BNP has a 6.57 odds of short term all cause mortality [13]
- An elevated lactate leads to 9.05 odds of PE related mortality [14]
- Beneficial for short term risk stratification
- POCUS is an alternative to formal transthoracic echocardiogram (TTE) if TTE is unavailable
- Goal is to evaluate for RV dysfunction as these signs are predictive of mortality
- RV dilation (RV:LV ratio in diastole >0.9) [15] [16]
- D sign (Left ventricular septal wall flattening)
- McConnell's Sign (Mid-RV wall akinesis with hyperdynamic apex)
- Tricuspid Annular Plane Systolic Excursion (TAPSE), <1.6cm is abnormal [17] [18]
- Often obtained to rule out other etiologies of chest pain and dyspnea
- Hampton's Hump
- Can be confused for a peripheral pneumonia as a wedge shaped peripheral opacity that indicates the presence of a pulmonary infarct
- Westermark's Sign
- A focal area of oligemia or reduced blood flow and increased lucency distal to the pulmonary embolism
- PE's can be associated with ECG changes that indicate acute pulmonary hypertension and right heart strain
- Abnormal in 70% of patients with a PE, however nonspecific [20]
- Sinus tachycardia
- Most common arrhythmia associated with PE
- Symmetric T wave inversions in the anterior leads (V1-V4)
- McGinn-White S1Q3T3 pattern
- Incomplete or complete right bundle branch block
- ST elevations in aVR
- Atrial fibrillation
Classification
- Both the ESC and the AHA/ACC proposed classification of patients with acute PE into categories based on their potential risk for adverse outcomes
- ESC 2019 Guidelines: Updated the 2011 AHA/ACC tool by splitting the intermediate or previously referred to as "submassive" patient group into those that present with low-risk features and those that present with high-risk features while maintaining stable hemodynamics.
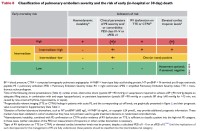
ESC 2019 PE Classification
- AHA/ACC 2026 Guidelines: A new, 5 tier, non-validated tool using an A-E category system with multiple subcategories is presented in a way to capture higher risk patients who may not have underlying RV dysfunction or cardiac biomarker abnormalities but appear to have a higher risk for adverse outcomes as noted in their proposed D group
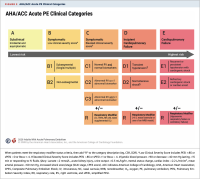
AHA 2026 PE Classification
- Categorization of PE patients allows for guidance in management decisions
Management
Anticoagulation
- Anticoagulation is the cornerstone of PE management and should be started in the ED
- If bleeding risk is very high, based on tools such as VTE Bleed or RIETE, consider discussing anticoagulation strategies with hematology, pulmonology, or PERT (if available at your institution) prior to initiating anticoagulation
| Name
|
Apixaban PO
|
Rivaroxaban PO
|
Dabigatran PO
|
LMWH SC
|
Unfractionated Heparin IV
|
Coumadin PO
|
| Initial Dose
|
- 10mg twice daily for 1 week, then 5mg twice daily
|
- 15mg twice daily for 3 weeks, then 20mg once daily
|
- Initiate heparin treatment for 5-10 days; then 150mg twice daily
|
|
- 80 units/kg bolus; then 18 units/kg/hr continuous infusion
|
|
| Indication
|
- Preferred oral treatment
- All CKD stages
|
- Preferred oral treatment
- CKD Stages II-III (GFR 30-90 mL/min)
|
- CKD Stages II-III (GFR 30-90 mL/min)
|
- Preferred parenteral treatment
- Can be used in patients undergoing advanced therapies
|
- Can be used in patients undergoing advanced therapies
- Patients with mechanical prosthetic heart valve
|
- Patients with confirmed anti-phospholipid syndrome
- Patients with mechanical prosthetic heart valve
|
| Contraindications
|
- Pregnancy
- Breastfeeding
- Child-Pugh Class C Liver Disease
|
- CKD Stage V (GFR <15mL/min)
- Pregnancy
- Breastfeeding
- Child-Pugh Class C Liver Disease
|
- CKD Stage IV-V (GFR <30mL/min)
- Pregnancy
- Breastfeeding
- Child-Pugh Class C Liver Disease
|
|
|
|
| Dose Adjustments
|
|
|
|
- If BMI >40kg/m2, reduce dose (0.8mg/kg BID of enoxaparin)
- If Stage IV or greater CKD (GFR<30 mL/min), adjust to 1mg/kg QD
|
|
- Consider starting at 2.5mg PO if frail, elderly, malnourished, or with a history of liver disease
|
- Duration
- 3-6 mo, if time limited risk factor (post-op, trauma, estrogen use)
- 6 mo to life, if idiopathic etiology or recurrent
Advanced Therapies
- Systemic thrombolytics, catheter directed therapy, and less often surgical embolectomy may be considered for specific patients with acute PE, typically in categories C-E in the AHA/ACC guidelines or the intermediate-high risk/high risk in ESC guidelines
- However, decisions to pursue these therapies should be made with multidisciplinary specialty input
- Thrombolytics
- Thrombolytic therapies are a group of IV medications that activate fibrinolysis and break up clots
- In general, should only be reserved for patients in categories D/E or High risk, however some evidence suggests it may be beneficial for specific patients within category C3 [21] [22] [23]
- Thrombolytics should NOT be used over anticoagulation due to increased risk of major bleeding and ICH in patients within categories A-C2 [24] [25]
- Thrombolytic dosing is debated, however current standard dosing of rt-PA (alteplase) is 100mg IV over 2hrs
- Some evidence supports 25-50mg IV tPA,[26] [27] [28] highlighting similar efficacy and a lower bleeding risk, but no high quality trials have definitively proven this
- PEITHO-3 trial currently ongoing and hopes to elucidate this question
- Tenecteplase, while studied in certain trials, has not been FDA approved for PE thrombolysis, and has no head to head data comparing it with tPA [29] [30]
- Thrombolytics in Cardiac Arrest
- For patients in cardiac arrest with a presumed PE, thrombolytics may be considered, but there is no clear benefit and a paucity of evidence [31]
- Duration of CPR after lytic administration is not quantified, however best estimates are to continue high quality CPR for 30-60min after administration of thrombolytic medication
- Catheter Directed Therapies
- Catheter directed therapies continue to be studied for varying PE classifications with wide heterogeneity in methodology, leading to difficulty comparing treatment strategies
- Generally considered for patients in categories C-E and often on a case by case basis
- Mechanical thrombectomy
- Catheter-directed thrombolysis
- Combination of mechanical thrombectomy and catheter based thrombolytic administration
- Surgical Embolectomy
- Efficacy of surgical embolectomy vs anticoagulation alone has not been studied
- Majority of evidence is retrospective and often for patients who have had CPR and as a salvage therapy after systemic thrombolytics
- IVC Filter
- IVC filters can be used when standard anticoagulation therapy is contraindicated or when patients develop recurrent PE despite being on anticoagulation
Supportive care
- Oxygen therapy
- Hypoxemia (SpO2<90%) causes hypoxemic vasoconstriction, worsening acute pulmonary hypertension
- Target supplemental O2 to SpO2≥90%
- Be cautious about intubation as the increase in intrathoracic pressure from positive pressure can worsen RV preload and precipitate cardiovascular collapse
- Fluids
- Small (250-500mL) fluid boluses may be used as part of resuscitation in patients who are hemodynamically unstable
- Excessive IV fluids can worsen RV dilation and further compress LV, worsening hemodynamics
- Vasopressors
- May be used once fluids are no longer helpful
- Norepinephrine is generally first line
- Has a favorable SVR/PVR ratio with doses < 15 μg/min
- Vasopressin is a second line agent
- Consider adding once norepinephrine doses exceed 15 μg/min, as norepi at higher doses can lead to an increase in PVR
Disposition
- 20-30% of patients with a PE can be discharged from the ED, presuming they are able to start anticoagulation and have a stable social situation in which they are able to return for appropriate follow-up with an outpatient provider
- Hestia Criteria [32] can be used to guide decision making for patients who are safe to discharge from the ED
Prognosis
The Pulmonary Embolism Severity Index (PESI)[33]
| Prognosis Variable
|
Points Assigned
|
| Demographics |
|
| Age |
+Age in years
|
| Male |
+10
|
| Comorbid Conditions |
|
| Cancer |
+30
|
| Heart Failure |
+10
|
| Chronic Lung Disease |
+10
|
| Clincal Findings |
|
| Pulse >110 b/min |
+20
|
| sBP < 100 |
+30
|
| RR > 30 |
+20
|
| Temp <36 C |
+20
|
| AMS |
+60
|
| Art O2 Saturation <90% |
+20
|
| Risk Class
|
30-Day Mortality
|
Total Point Score
|
| I |
1.60% |
<65
|
| II |
3.50% |
66-85
|
| III |
7.10% |
86-105
|
| IV |
11.40% |
106-125
|
| V |
23.90% |
>125
|
Enoxaparin 1 mg/kg SC q12h SC — Preferred in cancer, liver disease, coagulopathy, pregnancy
Heparin (UFH) 80 units/kg IV bolus, then 18 units/kg/hr continuous infusion IV drip — Short half-life; preferred if considering thrombolytics or bleeding risk
Rivaroxaban 15 mg PO BID x3 weeks, then 20 mg PO daily PO — Preferred if parenteral therapy to be avoided
Apixaban 10 mg PO BID x1 week, then 5 mg PO BID PO
Additional Topics
- PERT Teams
- Pulmonary embolism response team (PERT) is a multidisciplinary group that provide real time expertise in management of patients at higher risk for adverse events in the setting of an acute PE
- Often composed of emergency medicine, pulmonology, critical care, interventional radiology, vascular surgery, cardiology, as well as nursing and pharmacy
- 60% of all PERT activations originate in the ED and have been shown to improve overall care and reduce disposition times, as well as facilitate advanced therapies [34]
- Clot in Transit
- A ‘clot in transit’, a free floating blood clot discovered within the cardiac chambers either on echocardiogram or CT, is found in 2-4% of patients with PE
- Leads to 2.26 OR of increased mortality [35]
- Some evidence to support that these patients fare better with systemic thrombolysis compared to anticoagulation alone [36]
- Special Populations
- Pulmonary Embolism in Pregnancy
- Renal Failure
- Patients with renal failure are at increased risk of both VTE as well as bleeding
- Treatment
- DOACs are preferred to VKA in Stage II-III CKD (GFR 30-89 ml/min) [37] [38] [39]
- Patients with Stage IV, V, or on renal replacement therapy were excluded from randomized trials, but data from US Renal Data System shows apixaban is as safe and effective as warfarin in Stage IV and higher CKD[40] [41]
- When LMWH is used, transition to once daily dosing due to extended half-life
- Morbid obesity
- Patients who are obese have less lean body mass, often leading to supratherapeutic anticoagulation when using standard LMWH dosing
- Evidence supports reduced dosing of LMWH to 0.8 mg/kg BID in BMI ≥40 kg/m2 with no clear increased thrombotic events, but less rate of major bleeding and lower rates of supratherapeutic events[42]
- Active Cancer
- Patients with cancer are at increased VTE risk
- Treatment for most stable patients is preferred with a DOAC, however LMWH may be indicated if;
- oral ingestion or gastrointestinal absorption is limited
- Severe thrombocytopenia related to chemotherapy
Calculators
A-a O₂ Gradient
Alveolar-arterial (A-a) O₂ Gradient
| Parameter
|
Value
|
| Age (years)
|
|
| FiO₂ (%)
|
|
| PaCO₂ (mmHg)
|
|
| PaO₂ (mmHg)
|
|
| A-a Gradient
|
mmHg
|
| Expected A-a
|
mmHg (age-adjusted normal)
|
Interpretation
- Normal A-a gradient ≈ (Age/4) + 4 on room air
- Elevated A-a gradient suggests: V/Q mismatch, shunt, or diffusion impairment
- Normal A-a gradient + hypoxia suggests: hypoventilation or low FiO₂
|
References
- Formula: A-a = [FiO₂ × (Patm – PH2O)] – (PaCO₂/0.8) – PaO₂
- Kanber GJ, et al. The alveolar-arterial oxygen gradient in young and elderly men during air and oxygen breathing. Am Rev Respir Dis. 1968;97(3):376-381. PMID 5637791.
|
Wells Score for PE
Wells' PE Score Calculator
| Criteria
|
No
|
Yes
|
Points
|
| Clinical signs and symptoms of DVT (leg swelling, pain with palpation)
|
1
|
|
+3.0
|
| PE is #1 diagnosis OR equally likely
|
1
|
|
+3.0
|
| Heart rate >100 bpm
|
1
|
|
+1.5
|
| Immobilization (≥3 days) OR surgery in previous 4 weeks
|
1
|
|
+1.5
|
| Previous objectively diagnosed PE or DVT
|
1
|
|
+1.5
|
| Hemoptysis
|
1
|
|
+1.0
|
| Malignancy (treatment within 6 months or palliative)
|
1
|
|
+1.0
|
| Wells' Score
|
points
|
Three-Tier Model
| 0–1
|
Low Risk — 1.3% incidence of PE. Consider D-dimer to rule out. Consider PERC rule.
|
| 2–6
|
Moderate Risk — 16.2% incidence of PE. Consider high-sensitivity D-dimer or CTA.
|
| >6
|
High Risk — 37.5% incidence of PE. Consider CTA. D-dimer not recommended.
|
Two-Tier Model (Preferred by guidelines)
| 0–4
|
PE Unlikely — 12.1% incidence. Consider high-sensitivity D-dimer; if negative, stop workup.
|
| >4
|
PE Likely — 37.1% incidence. Consider CTA testing.
|
| References
|
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism. Thromb Haemost. 2000;83(3):416-420. PMID 10744147.
- van Belle A, Büller HR, Huisman MV, et al. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006;295(2):172-179. PMID 16403929.
|
PERC Rule
PERC Rule Calculator
| Criteria
|
No (0)
|
Yes (+1)
|
| Age ≥50 years
|
1
|
|
| Heart rate ≥100 bpm
|
1
|
|
| SpO₂ <95% on room air
|
1
|
|
| Unilateral leg swelling
|
1
|
|
| Hemoptysis
|
1
|
|
| Recent surgery or trauma (within 4 weeks requiring hospitalization)
|
1
|
|
| Prior PE or DVT
|
1
|
|
| Hormone use (oral contraceptives, HRT, or estrogenic hormones)
|
1
|
|
| Positive Criteria
|
/ 8
|
Interpretation
| Score = 0
|
PERC Negative — If pre-test probability is ≤15%, PE is effectively ruled out. No further workup needed (sensitivity 97.4%, NPV 99.5%).
|
| Score ≥ 1
|
PERC Positive — Cannot rule out PE by PERC alone. Consider D-dimer, Wells' score, or CTA based on clinical suspicion.
|
External Links
References
- ↑ Kearon C. Natural history of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I22-I30. doi:10.1161/01.CIR.0000078464.82671.78
- ↑ Lautz TB, Abbas F, Walsh SJ, et al. Isolated gastrocnemius and soleal vein thrombosis: should these patients receive therapeutic anticoagulation?. Ann Surg. 2010;251(4):735-742. doi:10.1097/SLA.0b013e3181c1ae95
- ↑ Macdonald PS, Kahn SR, Miller N, Obrand D. Short-term natural history of isolated gastrocnemius and soleal vein thrombosis. J Vasc Surg. 2003;37(3):523-527. doi:10.1067/mva.2003.149
- ↑ Freund Y, Cohen-Aubart F, Bloom B. Acute Pulmonary Embolism: A Review. JAMA. 2022;328(13):1336-1345. doi:10.1001/jama.2022.16815
- ↑ Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation. 2023;147(8):e93-e621. doi:10.1161/CIR.0000000000001123
- ↑ Schultz J, Giordano N, Zheng H, et al. EXPRESS: A Multidisciplinary Pulmonary Embolism Response Team (PERT) - Experience from a national multicenter consortium. Pulm Circ. Published online January 11, 2019. doi:10.1177/2045894018824563
- ↑ Walls R, Hockberger R, Gausche-Hill M, Erickson TB, & Wilcox SR. (2022). Rosen's Emergency Medicine - Concepts and Clinical Practice E-Book (10th ed.). Elsevier - OHCE.
- ↑ Creager MA, Barnes GD, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026;153(12):e977-e1051. doi:10.1161/CIR.0000000000001415
- ↑ American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Thromboembolic Disease:, Wolf SJ, Hahn SA, et al. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department With Suspected Acute Venous Thromboembolic Disease. Ann Emerg Med. 2018;71(5):e59-e109. doi:10.1016/j.annemergmed.2018.03.006
- ↑ Creager MA, Barnes GD, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026;153(12):e977-e1051. doi:10.1161/CIR.0000000000001415
- ↑ Lu Y, Lorenzoni A, Fox JJ, et al. Noncontrast perfusion single-photon emission CT/CT scanning: a new test for the expedited, high-accuracy diagnosis of acute pulmonary embolism. Chest. 2014;145(5):1079-1088. doi:10.1378/chest.13-2090
- ↑ El-Menyar A, et al. Elevated serum cardiac troponin and mortality in acute pulmonary embolism: Systematic review and meta-analysis. Respiratory Medicine, 2019; 157, 26-35
- ↑ Coutance G, et al. Prognostic value of brain natriuretic peptide in acute pulmonary embolism. Crit Care. 2008;12(4):R109. doi:10.1186/cc6996
- ↑ Wang Y, et al. Prognostic role of elevated lactate in acute pulmonary embolism: A systematic review and meta-analysis. Phlebology. 2022;37(5):338-347. doi:10.1177/02683555221081818
- ↑ Mavromanoli AC et al. Recovery of right ventricular function after intermediate-risk pulmonary embolism: results from the multicentre Pulmonary Embolism International Trial (PEITHO)-2. Clin Res Cardiol. 2023;112(10):1372-1381. doi:10.1007/s00392-022-02138-4
- ↑ Meyer G et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-1411. doi:10.1056/NEJMoa1302097
- ↑ Mavromanoli AC et al. Recovery of right ventricular function after intermediate-risk pulmonary embolism: results from the multicentre Pulmonary Embolism International Trial (PEITHO)-2. Clin Res Cardiol. 2023;112(10):1372-1381. doi:10.1007/s00392-022-02138-4
- ↑ Lobo JL, et al. Prognostic significance of tricuspid annular displacement in normotensive patients with acute symptomatic pulmonary embolism. J Thromb Haemost2014; 12: 1020–7.
- ↑ http://www.thepocusatlas.com/right-ventricle
- ↑ Shopp JD, et al. Findings From 12-lead Electrocardiography That Predict Circulatory Shock From Pulmonary Embolism: Systematic Review and Meta-analysis. Acad Emerg Med. 2015;22(10):1127-1137.doi:10.1111/acem.12769
- ↑ Marti C et al. Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta-analysis. Eur Heart J. 2015;36(10):605-614. doi:10.1093/eurheartj/ehu218
- ↑ Hao Q et al. Thrombolytic therapy for pulmonary embolism. Cochrane Database Syst Rev. 2015;(9):CD004437. Published 2015 Sep 30. doi:10.1002/14651858.CD004437.pub4
- ↑ Chatterjee S et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. 2014;311(23):2414-2421. doi:10.1001/jama.2014.5990
- ↑ Chatterjee S et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. 2014;311(23):2414-2421. doi:10.1001/jama.2014.5990
- ↑ Silver MJ et al. Incidence of Mortality and Complications in High-Risk Pulmonary Embolism: A Systematic Review and Meta-Analysis. J Soc Cardiovasc Angiogr Interv. 2023;2(1):100548. Published 2023 Jan 27. doi:10.1016/j.jscai.2022.100548
- ↑ Guru PK et al. Ultra-Low-Dose Systemic Tissue Plasminogen Activator in High-Risk Submassive Pulmonary Embolism. Mayo Clin Proc. 2022;97(6):1158-1163. doi:10.1016/j.mayocp.2022.02.011
- ↑ Charif F et al. Low dose peripheral systemic thrombolysis for treatment of intermediate-high risk acute pulmonary embolism: a case series. Eur Heart J Case Rep. 2022;6(10):ytac417. Published 2022 Oct 12. doi:10.1093/ehjcr/ytac417
- ↑ Aykan AÇ et al. Reduced-Dose Systemic Fibrinolysis in Massive Pulmonary Embolism: A Pilot Study. Clin Exp Emerg Med. 2023;10(3):280-286. doi:10.15441/ceem.23.015
- ↑ Kline JA et al. Treatment of submassive pulmonary embolism with tenecteplase or placebo: cardiopulmonary outcomes at 3 months: multicenter double-blind, placebo-controlled randomized trial. J Thromb Haemost. 2014;12(4):459-468. doi:10.1111/jth.12521
- ↑ Konstantinides SV et al. Impact of Thrombolytic Therapy on the Long-Term Outcome of Intermediate-Risk Pulmonary Embolism. J Am Coll Cardiol. 2017;69(12):1536-1544. doi:10.1016/j.jacc.2016.12.039
- ↑ Cao D et al. Part 10: Adult and Pediatric Special Circumstances of Resuscitation: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025;152(16_suppl_2):S578-S672. doi:10.1161/CIR.0000000000001380
- ↑ Zondag et al. Hestia criteria can discriminate high- from low-risk patients with pulmonary embolism. European Respiratory Journal. 2013; 41:588-592.
- ↑ Aujesky D, Obrosky DS, Stone RA, et al. Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med. 2005;172:1041-1046.
- ↑ Schultz J et al. EXPRESS: A Multidisciplinary Pulmonary Embolism Response Team (PERT) - Experience from a national multicenter consortium. Pulm Circ. Published online January 11, 2019. doi:10.1177/2045894018824563
- ↑ Kobayashi T et al. Contemporary Management and Outcomes of Patients With High-Risk Pulmonary Embolism. J Am Coll Cardiol. 2024;83(1):35-43. doi:10.1016/j.jacc.2023.10.026
- ↑ Islam M et al. Right Heart Thrombi: Patient Outcomes by Treatment Modality and Predictors of Mortality: A Pooled Analysis. J Intensive Care Med. 2019;34(11-12):930-937. doi:10.1177/0885066618808193
- ↑ Alhousani M et al. Using oral anticoagulants among chronic kidney disease patients to prevent recurrent venous thromboembolism: A systematic review and meta-analysis. Thromb Res. 2021;198:103-114. doi:10.1016/j.thromres.2020.11.036
- ↑ Chen HY et al. Efficacy and Safety of Direct Oral Anticoagulants vs Warfarin in Patients with Chronic Kidney Disease and Dialysis Patients: A Systematic Review and Meta-Analysis. Clin Drug Investig. 2021;41(4):341-351. doi:10.1007/s40261-021-01016-7
- ↑ Parker K et al. A systematic review of the efficacy and safety of anticoagulants in advanced chronic kidney disease. J Nephrol. 2022;35(8):2015-2033. doi:10.1007/s40620-022-01413-x
- ↑ Ellenbogen MI et al. Safety and effectiveness of apixaban versus warfarin for acute venous thromboembolism in patients with end-stage kidney disease: A national cohort study. J Hosp Med. 2022;17(10):809-818. doi:10.1002/jhm.1292
- ↑ Fatima H et al. Safety and Efficacy of Apixaban vs Warfarin in Patients With Stage 4 and 5 Chronic Kidney Disease: A Systematic Review. Cureus. 2022;14(10):e30230. Published 2022 Oct 12. doi:10.7759/cureus.30230
- ↑ Liu J et al. Strategies involving low-molecular-weight heparin for the treatment and prevention of venous thromboembolism in patients with obesity: A systematic review and meta-analysis. Front Endocrinol (Lausanne). 2023;14:1084511. Published 2023 Mar 8. doi:10.3389/fendo.2023.1084511







