Background
- Characterized by diminished blood flow through the vertebral or basilar arteries
- The two vertebral arteries originally branch proximally from subclavian, travel through vertebrae, and distally join to become basilar artery
- Symptoms result from diminished circulation to the posterior brain, brainstem and cerebellum.
- Head-turning can cause ipsilateral vertebral artery to temporarily occlude
- If contralateral vertebral artery is stenotic, may lead to syncope (known as Bow hunter's syndrome[1])
- Head extension may also provoke symptoms
- Neurologic symptoms tend to not present when one vertebral artery remains patent[2]
- Symptoms may result secondary to arterial plaques, arterial dissection, compressive lesions, or subclavian steal (see below). *Posterior strokes encompass 20-30% of all strokes[3]
- Cervical osteophytes can also directly compress vertebral arteries and cause VBI symptoms[4].
Bow hunter's syndrome (Rotational vertebral artery compression)
- Head turning causes temporary occlusion of the ipsilateral vertebral artery. VBI results if the contralateral vertebral artery has a fixed occlusion[5]. Improvement of symptoms in neutral position is considered pathognomonic[6]
- Stenotic lesion in the subclavian, located proximal to the vertebral artery--> reversed flow of blood in the vertebral artery when superimposed with increased arm activity(4).
Clinical Features
Symptoms
Differential Diagnosis
- Vestibular/otologic
- Neurologic
- Other
Evaluation
Work-up
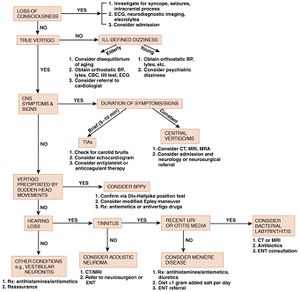
Diagnostic algorithm Vertigo
- Glucose check
- Full neuro exam
- TM exam
- CTA or MRA (diagnostic study of choice) of the neck/brain if symptoms consistent with central cause
| Test
|
Sensitivity
|
| HINTS |
100%
|
| MRI (24hrs) |
68.40%[7]
|
| MRI (48hrs) |
81%[7]
|
| CT non con |
26%[8]
|
- Proposed as method of distinguishing peripheral cause from cerebellar/brain stem CVA in the Emergency Department population [9][10][11]
Inclusion Criteria
- HINTS exam should only be used in patient with acute persistent vertigo, nystagmus, and a normal neurological exam.
- HINTS exam, when done correctly, has high sensitivity and specificity in distinguishing peripheral vs central etiologies of vertigo
- Note that the original study was done by neuro-ophthalmologists in a differentiated patient base. This exam has not been studied in a large ED population yet
The 3 components of the HINTS exam include:
| HINTS Test
|
Reassuring Finding
|
| Head Impulse Test |
Abnormal (corrective saccade)
|
| Nystagmus |
Unidirectional, horizontal
|
| Test of Skew |
No skew deviation
|
- Always use correct terminology; "HINTS negative" does not convey a clear interpretation. State "HINTS central" or "HINTS peripheral" as suggested in literature
- If able, specify the exact exam finding as shown by chart above
Head Impulse Test
Test of vestibulo-ocular reflex function
- Have patient fix their eyes on your nose
- Move their head rapidly in the horizontal plane to the left and right
- When the head is turned towards the normal side, the vestibular ocular reflex remains intact and eyes continue to fixate on the visual target
- When the head is turned towards the affected side, the vestibular ocular reflex fails and the eyes make a visible corrective saccade to re-fixate on the visual target [12][13]
- Normally, a functional vestibular system will identify any movement of the head position and instantaneously correct eye movement accordingly so that the center of the vision remains on a target.
- This reflex fails in peripheral causes of vertigo affecting the vestibulocochlear nerve unilaterally; thus, failure of the reflex unilaterally is reassuring (since the cause is peripheral)
- Note that in central causes of vertigo, test may show normal reflex response OR failure of the reflex BILATERALLY
Nystagmus
- Observation for nystagmus in primary, right, and left gaze
- No nystagmus (normal) or only horizontal unilateral nystagmus (fast direction only in one direction) is reassuring
- Any other type of nystagmus is abnormal, including vertical or bidirectional nystagmus
Test of Skew
- Have patient look at your nose with their eyes and then cover one eye
- Then rapidly uncover the eye and quickly look to see if the eye moves to re-align.
- Repeat with on each eye
- Skew deviation is a fairly specific predictor of brainstem involvement in patients with acute vestibular syndrome. The presence of skew may help identify stroke when a positive head impulse test falsely suggests a peripheral lesion.
- Skew is also known vertical dysconjugate gaze and is a sign of a central lesion
- A positive HINTS exam: 100% sensitive and 96% specific for the presence of a central lesion.
- The HINTS exam was more sensitive than general neurological signs: 100% versus 51%.
- The sensitivity of early MRI with DWI for lateral medullary or pontine stroke was lower than that of the HINTS examination (72% versus 100%, P=0.004) with comparable specificity (100% versus 96%, P=1.0).
- If any of the above 3 tests are consistent with CVA obtain full work-up (including MRI)
Management
Medical management
Surgical management
- Endarterectomy
- Bypass grafting
- Stenting
Disposition
See Also
External Links
References
- ↑ #Go G, Hwang S-H, Park IS, Park H. Rotational Vertebral Artery Compression : Bow Hunter’s Syndrome. Journal of Korean Neurosurgical Society. 2013;54(3):243-245. doi:10.3340/jkns.2013.54.3.243.
- ↑ Ibrahim Alnaami, Muzaffer Siddiqui, and Maher Saqqur, “The Diagnosis of Vertebrobasilar Insufficiency Using Transcranial Doppler Ultrasound,” Case Reports in Medicine, vol. 2012, Article ID 894913, 3 pages, 2012. doi:10.1155/2012/894913.
- ↑ Ibrahim Alnaami, Muzaffer Siddiqui, and Maher Saqqur, “The Diagnosis of Vertebrobasilar Insufficiency Using Transcranial Doppler Ultrasound,” Case Reports in Medicine, vol. 2012, Article ID 894913, 3 pages, 2012. doi:10.1155/2012/894913.
- ↑ Tintinalli
- ↑ #Go G, Hwang S-H, Park IS, Park H. Rotational Vertebral Artery Compression : Bow Hunter’s Syndrome. Journal of Korean Neurosurgical Society. 2013;54(3):243-245. doi:10.3340/jkns.2013.54.3.243.
- ↑ #Go G, Hwang S-H, Park IS, Park H. Rotational Vertebral Artery Compression : Bow Hunter’s Syndrome. Journal of Korean Neurosurgical Society. 2013;54(3):243-245. doi:10.3340/jkns.2013.54.3.243.
- ↑ 7.0 7.1 http://www.cnsuwo.ca/ebn/downloads/cats/2010/CNS-EBN_cat-document_2010-07-JUL-30_a-negative-dwi-mri-within-48-hours-of-stroke-symptoms-ruled-out-anterior-circulation-stroke_4494E.pdf
- ↑ Chalela JA, Kidwell CS, Nentwich LM, et al. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet. 2007;369:293–8.
- ↑ http://ec.libsyn.com/p/a/d/d/add761f2a2847ea5/hints-exam.pdf?d13a76d516d9dec20c3d276ce028ed5089ab1ce3dae902ea1d01c0873ed8cc5fe910&c_id=2502227
- ↑ http://www.ncbi.nlm.nih.gov/pubmed/18541870
- ↑ http://hwcdn.libsyn.com/p/1/c/d/1cd6b38a89c178a1/diff-of-vertigo.pdf?c_id=2502226&expiration=1380995436&hwt=0a8bc67ea910e018a1543ebea192f668
- ↑ Barraclough K, Bronstein A. Vertigo. BMJ. 2009;339:b3493
- ↑ Kuo CH, Pang L, Chang R. Vertigo - part 1 - assessment in general practice. Aust Fam Physician. 2008;37(5):341-7
