Austere peritoneal dialysis
Overview
- Improvised PD has been done in resource-limited settings such as the earthquakes in Turkey in 1999 and Haiti in 2010
- Indications in the austere setting are the same in non-austere settings
- Consider contacting a nephrologist via telemedicine if available
- Effective for hyperkalemia, though much slower than hemodialysis
- Relatively ineffective for uremia and eliminating BUN
Indications
- See indications in AKI
- However, there are certain situations that are more likely in disaster or combat situations:
- Rhabdomyolysis from crush injuries
- Severe pediatric dehydration and AKI
- Toxin clearance
Contraindications
- No absolute contraindications
- Relative contraindications include:
- Recent abdominal surgery
- Diaphragmatic injury with communication into thoracic space
- Overlying diffuse abdominal wall infection
- Known severe peritoneal adhesions
- Patients with severe respiratory failure that may not do well with intraperitoneal fluid
Equipment Needed
- Types of possible peritoneal catheters:
- Flexible Tenckhoff catheter is gold standard, but not available in austere setting
- Rigid trocar, non-tunneled catheter
- Improvised: NGTs, suprapubic catheters, pediatric chest tubes, large bore central venous catheters ("Cordis"), pigtail catheters, 8-10 Fr Foley catheters
- Scalpel
- Lidocaine
- Sterile preparation, sterile equipment
- Ultrasound
Procedure
- Consider giving preprocedural antibiotics such as ertapenam before start
- Fungal coverage where suspected to be an issue
- Ensure sterile technique in creating dialysate
- Additionally, antibiotics such as cephalosporins can be added to each PD bag
- Improvised flexible
- Local anesthesia, then midline incise 2 cm below umbilicus
- Blunt dissect to linea alba, then puncture through linea alba with rigid catheter, and insert a small volume of dialysate under US guidance
- Insert a guidewire through the initial catheter, then dilate using Seldinger technique to final catheter
- Rigid catheter
- Local anesthesia to area just lateral to umbilicus
- Advance pointed trocar, directed caudal toward iliac fossa
- See reference for dedicated tunneled PD catheter insertion
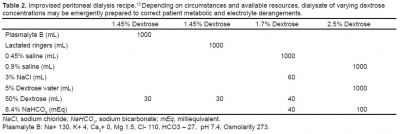
Dialysate
- Lactated Ringer's is the most readily available IVF and most similar to commercial dialysate fluid, but dextrose must be added to produce an osmotic dialysate
- Increasing dextrose concentration increases volume removal for hypervolemic patients
- Commercial dialysates usually have 1.5-4.25% dextrose
- Generally, dextrose concentrations increase 1% for every 20 mL of D50 per liter
- 500 units of heparin per liter can prevent PD catheter obstruction

Dialysis Process
- Attach threeway stop-cock to improvised catheter
- Infuse 1-2 L of dialysate in an adult, with dwell time of 2-4 hours, four times per day
- Smaller volume dwells of 500-1000 mL with 2-4 hours of dwell time may be more appropriate in the austere combat setting
- In pediatrics, give 10-20 mL/kg of dialysate, with total exchange time of 60-90 minutes, with 30-40 minutes of dwell time\
- Volume usage per day may range from 4 all the way to 70 L per day depending on targets of therapy
- Drainage is done by gravity or aspiration
- Frequently measure electrolytes and BUN/Cr, alongside collecting daily EKGs
Complications
- Hemorrhage, bowel or solid organ injury
- Peritonitis, including fungal peritonitis not otherwise covered by prophylactic antibiotics
- Dialysate leakage, especially in abdominal surgical patients with newly healing abdominal wounds
- Hydrothorax
- Catheter obstruction
References
- Gorbatkin C, Bass J, Finkelstein F, Gorbatkin S. Peritoneal Dialysis in Austere Environments: An Emergent Approach to Renal Failure Management. West J Emerg Med. 2018 May;19(3):548-556.