Shoulder dislocation
Background



- Humerus separates from the scapula at the glenohumeral joint
- Partial dislocation of the shoulder is referred to as subluxation
- Dislocation duration inversely correlated with likelihood of successful ED reduction
Shoulder dislocation types
- Anterior shoulder dislocation (~95%)
- Posterior shoulder dislocation (~5%)
- Inferior shoulder dislocation (<1%)
Clinical Features
- Shoulder pain
- Decreased shoulder range of motion
Comparison of Shoulder Dislocation Clinical Features
| Finding | Anterior (~95%) | Posterior (~5%) | Inferior (<1%) |
|---|---|---|---|
| Arm position | Arm maintained in abduction and external rotation | Posterior aspect of shoulder unusually prominent | Humerus fully abducted / Hand on or behind head |
| Shoulder appearance | Loss of normal rounded appearance with stretching of the deltoid muscle (i.e., "squared off") | Anterior aspect of shoulder appears flattened | |
| Range of motion | Difficulty touching affected arm to contralateral shoulder due to pain | Inability to rotate or abduct affected arm | Humeral head palpable in axilla or lateral chest wall |
| Mechanism | Most common; range of mechanisms | Forceful internal rotation and adduction (e.g., blow to anterior shoulder, seizure, eletric shock) | Forceful hyper-abduction of arm |
Differential Diagnosis
Shoulder and Upper Arm Diagnoses
Traumatic/Acute:
- Shoulder Dislocation
- Clavicle fracture
- Humerus fracture
- Scapula fracture
- Acromioclavicular joint injury
- Glenohumeral instability
- Rotator cuff tear
- Biceps tendon rupture
- Triceps tendon rupture
- Septic joint
Nontraumatic/Chronic:
- Rotator cuff tear
- Impingement syndrome
- Calcific tendinitis
- Adhesive capsulitis
- Biceps tendinitis
- Subacromial bursitis
- Cervical radiculopathy
Refered pain & non-orthopedic causes:
- Referred pain from
- Neck
- Diaphragm (e.g. gallbladder disease)
- Brachial plexus injury
- Axillary artery thrombosis
- Thoracic outlet syndrome
- Subclavian steal syndrome
- Pancoast tumor
- Myocardial infarction
- Pneumonia
- Pulmonary embolism
Evaluation
Workup
- Plain film X-ray
- Include anteroposterior, scapular Y, and axillary views
- Associated fractures include:
- Hills-Sachs: cortical depression in the humeral head
- Bankart: glenoid labrum disruption with bony avulsion
- Humeral greater tuberosity fracture
- Consider joint ultrasound
Diagnosis
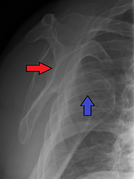
Anterior shoulder dislocation on Y-view

Anterior shoulder dislocation with fracture





Management
Reduction
- Do not attempt to reduce chronic dislocations (>4 weeks) in ED due to risk of arterial injury - these require reduction in the OR
- Lower complications, equal pain control, and shorter ED stay with intra-articular lidocaine vs. procedural sedation[1]
- 20 mL of 1% lidocaine intra-articular injection
- See individual types for specific techniques:
Post-Reduction
- Post-reduction film to confirm
- Sling and swathe or shoulder immobilizer x1 week / until orthopedics follow-up
- Encourage daily range of motion exercises (minus abduction + external rotation) to prevent adhesive capsulitis
Disposition
- Uncomplicated dislocation can be discharged after reduction
Prognosis
- Recurrence rate around 27% if older than 30 years and 72% if younger than 23 years[2]
See Also
External Links
- Good all-round shoulder reduction technique lecture
- Keeping Up in EM Shoulder Reduction Video
- Merk Manual - Shoulder dislocations
References
- ↑ Intra-articular lignocaine versus intravenous analgesia with or without sedation for manual reduction of acute anterior shoulder dislocation in adults (Review) Cochrane Database Syst Rev. 2011 Apr 13;(4):CD004919 full text
- ↑ Watson S, Allen B, Grant JA. A Clinical Review of Return-to-Play Considerations After Anterior Shoulder Dislocation. Sports Health. 2016; 8(4):336-341.