Conjunctivitis
This page is for adult patients. For pediatric patients, see: conjunctivitis (peds)
Background
- Most common cause of acute red eye
- Viral infection is usual etiology (vs bacterial) in adults[1]
Conjunctivitis Types
Clinical Features
- Injected conjunctiva with peri-limbal sparing
- Rarely painful; more irritated
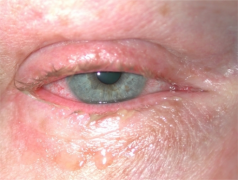
Conjunctivitis Images
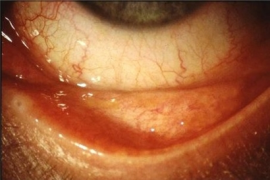
Acute allergic conjunctivitis
Chronic allergic conjunctivitis

Contact blepharoconjunctivitis










Differential Diagnosis
Unilateral red eye
- Nontraumatic
- Acute angle-closure glaucoma^
- Anterior uveitis
- Conjunctivitis
- Corneal erosion
- Corneal ulcer^
- Endophthalmitis^
- Episcleritis
- Herpes zoster ophthalmicus
- Inflamed pinguecula
- Inflamed pterygium
- Keratoconjunctivitis
- Keratoconus
- Nontraumatic iritis
- Scleritis^
- Subconjunctival hemorrhage
- Orbital trauma
- Caustic keratoconjunctivitis^^
- Corneal abrasion, Corneal laceration
- Conjunctival hemorrhage
- Conjunctival laceration
- Globe rupture^
- Hemorrhagic chemosis
- Lens dislocation
- Ocular foreign body
- Posterior vitreous detachment
- Retinal detachment
- Retrobulbar hemorrhage
- Traumatic hyphema
- Traumatic iritis
- Traumatic mydriasis
- Traumatic optic neuropathy
- Vitreous detachment
- Vitreous hemorrhage
- Ultraviolet keratitis
^Emergent diagnoses
^^Critical diagnoses
Bilateral red eyes
- Painful
- Painless
Evaluation
- Typically clinical
- However, a literature review attempting to differentiate bacterial vs viral concludes: No single symptom or sign differentiated the two conditions with high certainty.[2]
Clinical diagnosis of conjunctivitis^
| Bacterial | Viral | Allergic | |
|---|---|---|---|
| Bilateral | 50% | 25% | Mostly |
| Discharge | Mucopurulent | Clear, Watery | Cobblestoning, none |
| Redness | Yes | Yes | Yes |
| Pruritis | Rarely | Rarely | Yes |
| Increased Likelihood | Presence of mucopurulent discharge; otitis media | Concomitant pharyngitis; an enlarged preauricular node; contact with another person with red eye | NA |
| Additional | Treatment: Antibiotics | Treatment: Hygiene | Seasonal |
Management
- Viral infections - most common cause of conjunctivitis, but difficult to differentiate viral from bacterial
- Some clinicians treat all presentations as bacterial conjunctivitis
- Treatment considerations:
- Ointments - soothing effect, but interfere with vision
- Drops - no interference with vision
Antibiotics for Bacterial Causes
- Treatment for bacterial organisms is targeted toward S. aureus, S. pneumoniae, H. influenzae, Pseudomonas, N. gonorrhea, C. trachomatis
- Contact lens wearers should be given coverage for Pseudomonas with one of the fluoroquinolone drops.
- Contact lens wearers should be advised to not wear their contacts until asymptomatic
Bacterial Conjunctivitis
- Counsel patient/family on importance of hand hygiene/avoiding touching face to prevent spread!
- Apply warm or cool compresses (for comfort and cleansing) every 4 hours, followed by instillation of ophthalmic antibiotic solutions
These options do not cover gonococcal or chlamydial infections
- Polymyxin B/Trimethoprim (Polytrim) 2 drops every 6 hours for 7 days OR
- Erythromycin applied to the conjunctiva q6hrs for 7 days OR
- Levofloxacin 0.5% ophthalmic solution 1-2 drops every 2 hours for 2 days THEN every 6 hours for 5 days OR
- Moxifloxacin 0.5% ophthalmic 1-2 drops every 2 hours for 2 days THEN every 6 hours for 5 days OR
- Gatifloxacin 0.5% ophthalmic solution 1-2 drops every 2 hours for 2 days THEN 1 drop every 6 hours for 5 days OR
- Azithromycin 1% ophthalmic solution 1 drop BID for 2 days THEN 1 drop daily for 5 days
- Chloramphenicol 0.5% ophthalmic solution 1 drop QID for 7 days
NB: levofloxacin is preferred for contact lens wearers for coverage of pseudomonas. Advise not to wear contacts for duration of treatment
Pediatric
Same topical regimens as adults; erythromycin ointment preferred in neonates and young infants
- Erythromycin 0.5% ophthalmic ointment applied q6hrs x 7 days (preferred in neonates/infants) OR
- Moxifloxacin 0.5% ophthalmic 1 drop TID x 7 days OR
- Azithromycin 1% ophthalmic solution 1 drop BID x 2 days then daily x 5 days
Chlamydial
- Doxycycline 100mg PO BID for 7 days OR
- Azithromycin 1g (20mg/kg) PO one time dose
- Newborn Treatment: Azithromycin 20mg/kg PO once daily x 3 days or erythromycin PO 50 mg/kg/day in 4 divided doses for 14 days [3]
- Disease manifests 5 days post-birth to 2 weeks (late onset)
Gonococcal
- Due to increasing resistance, CDC recommends dual therapy with Ceftriaxone and Azithromycin (even if patient is negative for Chlamydia).
- Ceftriaxone 1g IM single dose PLUS
- Azithromycin 1g PO one dose
- Newborn Treatment:
- Prophylaxis: Erythromycin ophthalmic 0.5% x1
- Disease manifests 1st 5 days post delivery (early onset)
- Treatment Ceftriaxone 25-50mg IV or IM, max 125mg or cefotaxime single dose of 100 mg/kg (preferred if the patient has hyperbilirubinemia)
- Also requires evaluation for disseminated disease (meningitis, arthritis, etc.)
Contraindicated
- Corticosteroids have no benefit and can cause sight threatening injuries, especially in HSV or fungal causes of red eye
- Eye patching thought to exacerbate the infection
Disposition
- Outpatient treatment
See Also
References
- Mahmood, Narang. Diagnosis & management of acute red eye. Emerg Med Clin N Am 2008;26
- ↑ Johnson D, et al. "Does This Patient With Acute Infectious Conjunctivitis Have a Bacterial Infection" The Rational Clinical Examination Systematic Review. JAMA.2022;327(22):2231-2237. doi:10.1001/jama.2022.7687
- ↑ Johnson D, et al. "Does This Patient With Acute Infectious Conjunctivitis Have a Bacterial Infection" The Rational Clinical Examination Systematic Review. JAMA.2022;327(22):2231-2237. doi:10.1001/jama.2022.7687
- ↑ Zikic A, Schünemann H, Wi T, Lincetto O, Broutet N, Santesso N. Treatment of Neonatal Chlamydial Conjunctivitis: A Systematic Review and Meta-analysis. J Pediatric Infect Dis Soc. 2018 Aug 17;7(3):e107-e115. doi: 10.1093/jpids/piy060. PMID: 30007329; PMCID: PMC6097578.