Background
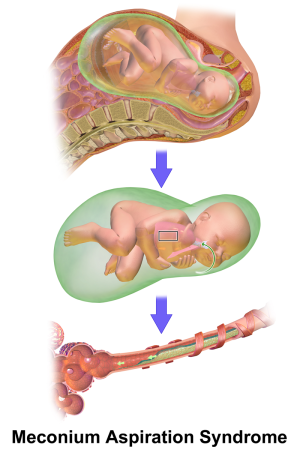
Image showing release of meconium into amniotic fluid (top), its progress into the mouth middle), and subsequently into the lung (C).
- Presentation ranges from mild respiratory distress to life-threatening respiratory failure
- Incidence is 2-10% of infants born through MSAF (meconium-stained amniotic fluid)
- Thought to be associated with fetal hypoxia and post-term delivery
- Causes hypoxemia and acidosis via airway obstruction, chemical irritation/inflammation, infection, and surfactant inactivation
- Associated with persistent pulmonary hypertension of the newborn (PPHN)
| Age
|
Pulse^
|
Respiratory Rate
|
Systolic BP
|
| Preterm < 1 kg |
120-160 |
30-60 |
36-58
|
| Preterm 1 kg |
120-160 |
30-60 |
42-66
|
| Preterm 2 kg |
120-160 |
30-60 |
50-72
|
| Newborn |
126-160 |
30-60 |
60-70
|
| Min of life |
Target sat^^
|
| 1 min |
60-65%
|
| 2 min |
65-70%
|
| 3 min |
70-75%
|
| 4 min |
75-80%
|
| 5 min |
80-85%
|
| 10 min |
85-95%
|
^Fever directly causes an increase in heart rate of 10 beats per minute per degree centigrade[2]
^^Hyperoxia can be harmful
Clinical Features
Differential Diagnosis
Newborn Problems
Evaluation

Chest X-ray of neonate with meconium aspiration.
Workup
- CXR
- Streaky, linear densities
- Hyperinflated lungs and flattened diaphragm
- Diffuse patchy opacities (may appear similar to RDS if severe)
- ABG
- Echocardiography
- Blood and sputum cultures
Diagnosis
- Clinical diagnosis based on the following:
- Evidence of meconium on infant
- Respiratory distress shortly after birth
- Characteristic CXR findings
- If intubation required, meconium visualized in trachea
- Ways to differentiate between other causes of respiratory distress in a neonate:
- Transient tachypnea of the newborn is more common in late preterm infants (34-37 weeks) and RDS in preterm infants, whereas MAS more common in postmature infants (>41 weeks)
- Delayed transition from fetal circulation symptoms improve more quickly than those of MAS
- Congenital cyanotic heart disease is differentiated by physical exam (murmurs, hepatomegaly), CXR (cardiac size/shape), and echocardiogram (cardiac anatomy and function)
Management
- Supportive care: see newborn resuscitation
- Adequate oxygenation and ventilation
- Supplemental oxygen to keep saturation >99% and PaO2 55-90
- Assisted ventilation with CPAP if FiO2 exceeds 0.4 to 0.5
- High frequency oscillatory ventilation or ECMO for those who fail conventional mechanical ventilation
- Goal PaCO2 50-55 mmHg
- Maintain blood pressure and perfusion
- Umbilical lines to monitor blood gases and BP
- Correct metabolic abnormalities
- Empiric antibiotics while awaiting culture results (because of difficulty differentiating between pneumonia initially)
- Surfactant administration for severe disease requiring mechanical ventilation, FiO2>0.5, and mean airway pressure >10-12
Disposition
Prevention
- Fetal heart rate monitoring intrapartum to reduce risk of fetal hypoxia
- Induction of labor after 41 weeks gestation to reduce postmature delivery
- Amnioinfusion with isotonic fluid to dilute thick meconium is NOT routinely recommended
See Also
External Links
References
.png)
